Risk stratification; high, moderate and low risk
Tutorial presented by Dr Jane Armstrong, GP in CTMUHB and Clinical Director for Primary Care.
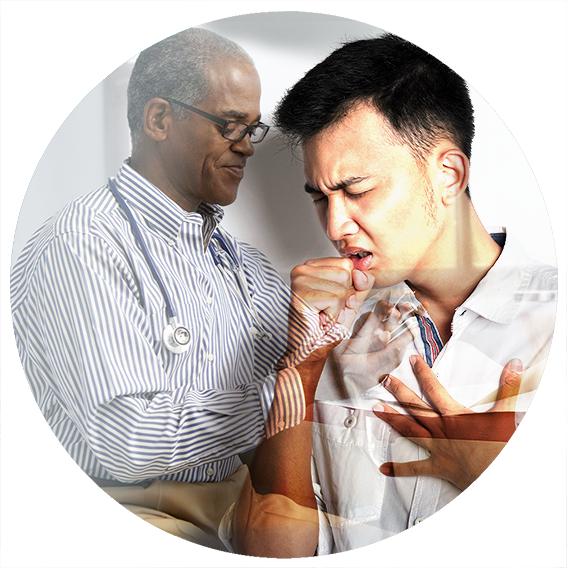
It’s difficult to know which patients may need admitting to hospital with COVID-19 due to the unpredictable nature of the condition. Infection can be mild, but the patient can also become critically unwell, and this can happen quickly.
Risk stratification can help ensure that the right people get the right care at the right time. People at increased risk are typically over the age of 65, or have co-morbidities, or are in the BAME (Black, Asian and Minority Ethnic) group. Oxygenation failure (low SpO2) is an independent risk factor for all patients. Ultimately, clinical judgment must aways supersede this guidance.
Low risk
- Any patient below age 65 years, do not have any co-morbidities, and their SpO2 is greater than or equal to 95%
Moderate risk
- Patients who are over the age of 65 years
- Patients with co-morbidities such as:
- diabetes
- cardiovascular disease
- respiratory disease
- active cancer treatment
- obesity
- Patients in the BAME group
- Patients with SpO2 above 92% and below 95%
High risk
- Any patients with SpO2 value less than or equal to 92%
- Any patient with an underlying diagnosis of COPD (or other respiratory disease) who has a SpO2 less than 88% or their SpO2 is more than 5% below their normal baseline
- Any high risk patient with SpO2 <95% with confusion, tachypnoea, tachycardia and vomiting that are too sick for management in a virtual ward
The rapid point-of-care COVID tests should be reserved for patients who fall in to the high or moderate risk category. The test should be undertaken ideally prior to being conveyed to hospital to ensure a COVID status is ascertained prior to admission, where a patient may be moved between sites and care homes to protect others, or in cases where the test result is likely to change the immediate management of the patient.
All other patients should be advised to have a routine COVID test in the community (with safety netting advice and self-isolation) to preserve rapid point-of-care testing strips to those who require it.
Risk stratification; high, moderate and low risk
Tutorial presented by Dr Jane Armstrong, GP in CTMUHB and Clinical Director for Primary Care.
It’s difficult to know which patients may need admitting to hospital with COVID-19 due to the unpredictable nature of the condition. Infection can be mild, but the patient can also become critically unwell, and this can happen quickly.
Risk stratification can help ensure that the right people get the right care at the right time. People at increased risk are typically over the age of 65, or have co-morbidities, or are in the BAME (Black, Asian and Minority Ethnic) group. Oxygenation failure (low SpO2) is an independent risk factor for all patients. Ultimately, clinical judgment must aways supersede this guidance.
Low risk
- Any patient below age 65 years, do not have any co-morbidities, and their SpO2 is greater than or equal to 95%
Moderate risk
- Patients who are over the age of 65 years
- Patients with co-morbidities such as:
- diabetes
- cardiovascular disease
- respiratory disease
- active cancer treatment
- obesity
- Patients in the BAME group
- Patients with SpO2 above 92% and below 95%
High risk
- Any patients with SpO2 value less than or equal to 92%
- Any patient with an underlying diagnosis of COPD (or other respiratory disease) who has a SpO2 less than 88% or their SpO2 is more than 5% below their normal baseline
- Any high risk patient with SpO2 <95% with confusion, tachypnoea, tachycardia and vomiting that are too sick for management in a virtual ward
The rapid point-of-care COVID tests should be reserved for patients who fall in to the high or moderate risk category. The test should be undertaken ideally prior to being conveyed to hospital to ensure a COVID status is ascertained prior to admission, where a patient may be moved between sites and care homes to protect others, or in cases where the test result is likely to change the immediate management of the patient.
All other patients should be advised to have a routine COVID test in the community (with safety netting advice and self-isolation) to preserve rapid point-of-care testing strips to those who require it.
Resources
 |
|---|
All Wales Guideline for the Management of patients with confirmed or suspected COVID-19 in the Community
More like this

The use of pulse oximeters as an advanced safety net for patients with COVID-19 in the community

Face to face assessment of patients by paramedics